Last updated April 23, 2024
Written by: Camden Malone, Global Health Policy Associate, United Nations Foundation
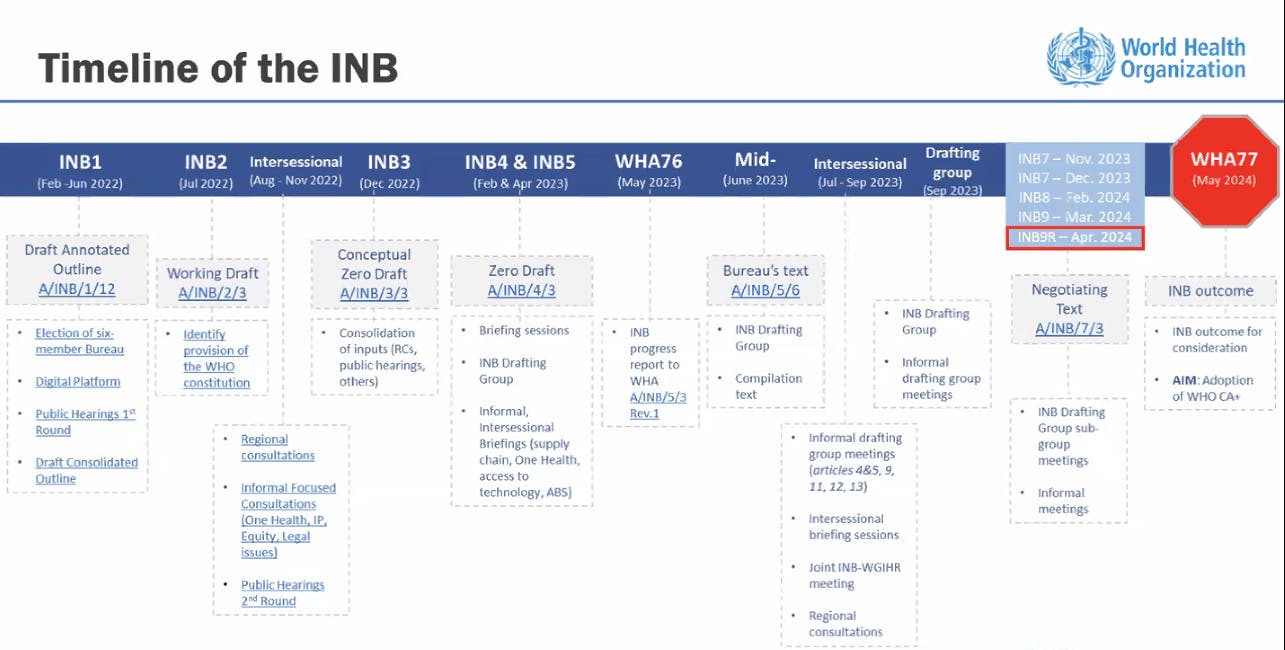
Over two years ago, ascending from the depths of the COVID-19 pandemic, world leaders committed to negotiating an innovative, legally-binding instrument to strengthen our collective pandemic preparedness, prevention, and response (PPPR). An ambitious timeline was set to draft and negotiate this Agreement, commonly referred to as the pandemic accord or pandemic treaty, in time for adoption at the 77th World Health Assembly (WHA) in May. However, after nine meetings of the Intergovernmental Negotiating Body (INB) – a group of representatives from WHO Member States tasked with reaching an agreement – their work remains unfinished.
Countries have come far in these negotiations, but not far enough. At what was intended to be their last session on March 28, delegates wrapped up the discussions in Geneva without a final deal struck and, hence, decided to reconvene on April 29.
Progress in recent months has been incremental. Line-by-line negotiations have been protracted, exemplified in a draft text that swelled to over 100 pages once countries incorporated their last proposed edits. The Bureau focused on text-based negotiations to reach a consensus, highlighting agreed text in green. This has proven to be no easy feat, especially given that the provisions of many Articles are interconnected, and thus, ‘greening’ one requires greening several others.
Now, with the May deadline looming, it appears the INB is pursuing a different approach. The latest draft text, shared by the INB Bureau on April 16, alludes to a potential Agreement consisting solely of a selective set of articles. In addition to the draft text, the Bureau also made public a draft WHA resolution to be considered during the Assembly. The resolution outlines possible modalities and a timeline for some of the more contentious items, a few detailed below, which would be deferred to a future track.
Many roadblocks in the negotiations reflect diverging views between high-income and low- and middle-income countries (LMICs).
On one hand, the Group for Equity, comprised of 34 LMICs, remains committed to ensuring that equity is mainstreamed across the entirety of the Agreement. These priorities include but are not limited to conditionalities for public research and development funding (Article 9), technology transfer (Article 11), and legally binding obligations to facilitate equitable diversification and supply of production of pandemic-related products (Articles 10 and 13). The Group has also called for Articles 19 and 20, on implementation and financing, to better reflect differences in countries’ capacities to implement the Agreement’s provisions (often referred to as Common But Differentiated Responsibilities or “CBDR”).
On the other hand, several delegations (primarily high-income countries) have maintained that the inclusion of CBDR, new financial mechanisms, and non-voluntary provisions, such as technology transfer and intellectual property waivers, are red lines that will draw few, if any, flexibilities during upcoming negotiations.
For all Member States alike, the WHO Pathogen Access and Benefit Sharing System (PABS-S) (Article 12) is the highest but most complex priority. Under the proposed mechanism, Parties would share pathogens and genetic sequence data across a WHO-coordinated laboratory network and publicly accessible databases recognized as part of the system. Draft provisions also state that in the event of a pandemic, manufacturers that produce medical countermeasures must contribute 10% free of charge and 10% at non-profit prices in “real-time,” but there is little specificity yet as to how this total 20% of supply will be equitably distributed between all Parties. Member States, civil society, and the private sector continue to debate what a negotiable PABS-S could look like.
Based on the proposed WHA resolution, outcomes for One Health and PABS will likely serve as placeholders for future instruments to be determined through Intergovernmental Working Groups (IGWGs). The timeline for these Articles would therein be extended for consideration at the next World Health Assembly in 2025 with final implementation proposed by May 2026. Member States are currently weighing options to determine whether these issues should be addressed through separate work streams or combined under one intergovernmental process. It also remains undecided to date if other sticking points, namely financing, are to be punted past this upcoming WHA as well.
Meanwhile, the fate of upcoming negotiations rests on the level of compromise brought to the table.
The mandate to compose robust commitments across the PPPR arc in a span of roughly two years is an immense challenge. As time shrinks, some blame for the emerging risk of spoils has been assigned to this idealistic timeline. True, the tight window, fraught political environment, and waning interest in PPPR pass no favors. An agreement is still possible, however, perhaps just with less ambition than originally anticipated. That ambition will need more time to play out as put forward in the WHA draft resolution.
In late-April of 1986, the world witnessed an unimaginable nuclear disaster in Chernobyl. Parallel to intensive emergency response efforts, countries negotiated and adopted the Convention on Early Notification of a Nuclear Accident in a span of six months.
In 2005, countries underwent efforts to negotiate comprehensive revisions to the International Health Regulations (IHR) to expand methods for controlling infectious disease outbreaks. It took only two years for the instrument to be adopted by every WHO Member State and entered into force. This year, Member States appear to be on track to deliver a new package of amendments to the IHR (2005) in a very similar timeframe.
The most pivotal documents enshrined in global governance were also agreed upon at an extraordinary pace. Out of the ashes of WWII, the UN Charter was conceived in only two months. A year later, the WHO Constitution was negotiated and signed in just six.
In times of crisis, diplomacy has proven to prevail. Although past achievements are not a prophesier, they do lend room for optimism. Indeed, given the context of COVID-19 and the potential for a future pandemic threat, there is an urgency for negotiators of this process to show similar resolve and craftiness.
The current draft resolution for WHA signals an Agreement to be adopted under Article 19 of the WHO Constitution, which lays a foundation similar to the Framework Convention on Tobacco Control (FCTC). This versatile governance structure enables negotiations of more complicated elements to continue for months, even years after its adoption. For example, the draft resolution suggests that tougher provisions could be put under Article 21 of the Constitution, allowing for an opt-in or opt-out modality for specific Articles of the accord.
The INB resumes their ninth and final meeting April 29 – May 10, with the goal of concluding substantive negotiations by May 5. As their work officially ends at this meeting’s gavel, Member States must agree on a clear approach to continue working on what could not be finalized in an initial Agreement.
Member States and relevant stakeholders will meet on May 3 to take stock of progress and determine a way forward as they approach the World Health Assembly in late-May. With steep barriers still to climb, delegations will have to make full productive use of their time and maintain good faith to reach consensus, an effort coined as the “spirit of Geneva.”
Camden Malone advances the global health agenda through engagement with UN Member States on a wide range of health policy issues, including universal health coverage, antimicrobial resistance, and pandemic preparedness, prevention, and response. Prior to the United Nations Foundation, Camden worked at the Permanent Mission of Costa Rica to the UN, covering intergovernmental negotiations related to health and human rights. Camden holds a master’s degree in International Affairs from the Colin Powell School for Civic and Global Leadership at the City College of New York; and a bachelor’s degree in History and Political Science from the College of Saint Rose.
To get the latest Global Health news from our experts, subscribe to our monthly newsletter.